
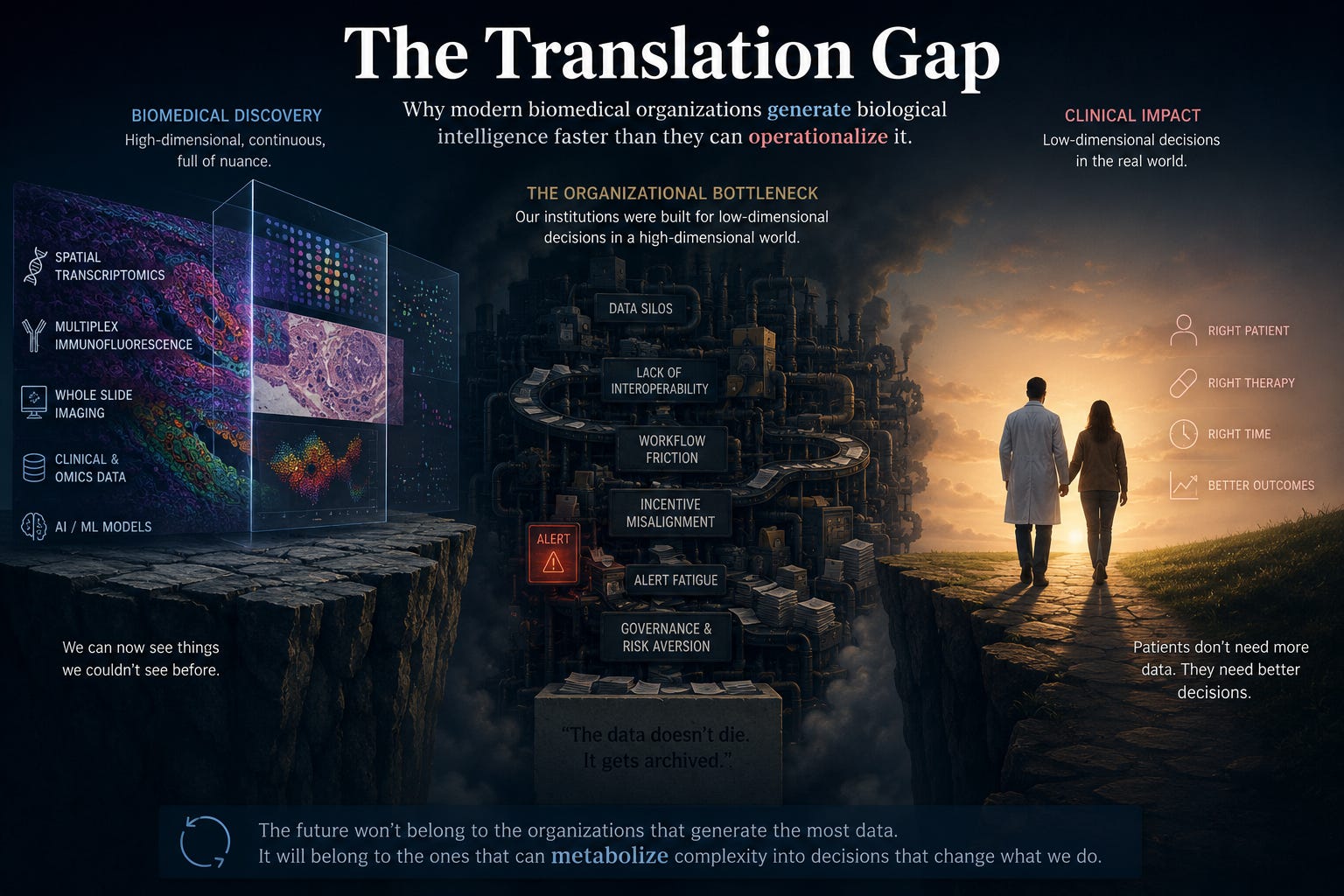
The Translation Gap
Why modern biomedical organizations generate biological intelligence faster than they can operationalize it

The biomarker was real.
The spatial signal was beautiful. The macrophage population appeared exactly where the biology predicted it should. We had spatial transcriptomics, multiplex immunofluorescence, historical correlations, conventional pathology validation. Months of work. Internal reviewers were impressed.
Everything worked.
Except the organization…
I remember the moment clearly. We were a team working with a spatial transcriptomics dataset: roughly twenty samples, a complete biomarker signature, historical data correlations, IHC for confirmation. The paper was halfway written. Everything was supposed to go well.
Then the last sample was contaminated. No drama, no blame. It happens.
“When will the next one be ready?” I asked, with the innocence of someone who still believes biology and logistics run on the same clock.
“In about a month, if everything goes smoothly,” the lab lead said.
As a physician, something in me already knew the answer: good in theory. Complicated in practice.
If you work in translational medicine, clinical development, or anywhere at the intersection of scientific discovery and clinical decision-making, you recognize this moment. Not as an anecdote. As a pattern, one that repeats itself, with different actors and different names, across nearly every organization that generates frontier science.
We call that pattern the translation gap. And in this piece I want to say something that rarely gets said directly: the gap is not primarily between science and patients. It lives inside our own organizations. And it is costing more than anyone wants to admit.
The problem everyone knows, but few name
In recent years, tissue biology has made an extraordinary leap. Platforms like Visium HD, COMET, and multiplex immunofluorescence panels now let us map more than forty markers simultaneously at subcellular resolution. We have solved, in practical terms, the historical trilemma between spatial resolution, transcriptomic depth, and analytical throughput.
We can now see things that were invisible a decade ago: how specific macrophages reprogram themselves at the tumor invasion front, which stromal cells physically block drug delivery, where the molecular conversations that drive acquired resistance are taking place.
And yet, more than 80% of AI initiatives in the pharmaceutical and clinical space remain trapped in what implementation scientists call “pilot purgatory”: projects that work in the lab, that generate impressive slides in steering committees, but that never change a single real clinical decision.
The question that deserves an honest answer is not technical. It is organizational: why can’t the organizations generating these findings actually use them?
Three cases everyone in this field should know
I don’t need to invent examples. The literature from the last five years is full of them.
The Epic Sepsis Model
Deployed across hundreds of U.S. hospitals, it reported an internal AUC of 0.83, a number that, on paper, inspires confidence. An independent external validation at the University of Michigan revealed that its real-world sensitivity was 33%. Two out of every three actual sepsis cases went undetected. And for every true positive, the system generated seven false alarms.
The consequences weren’t just statistical. Nursing staff, overwhelmed by alerts that carried no actionable clinical meaning, developed a documented pattern of ignoring the system altogether. Alert fatigue is not a metaphor. It’s an adaptive response to an environment that produces noise without signal.
IBM Watson for Oncology
Four billion dollars of investment. The goal was legitimate: personalized therapeutic recommendations in oncology. The problem was that the system was trained on hypothetical cases curated by a select group of specialists, not on the real-world heterogeneity of cancer patients. When the Danish National Cancer Center evaluated it prospectively, Watson agreed with local clinical judgment in just 33% of cases. In some scenarios, its recommendations were classified as clinically incorrect and unsafe. The project ended with the fragmented sale of assets at a fraction of development cost.
AI didn’t fail. The bridge between what the system learned and the world where it had to operate, that failed.
Google Health’s diabetic retinopathy screening in Thailand
This one may be the most instructive of the three, because the algorithm was genuinely good: AUC of 0.991, on par with an expert ophthalmologist. Deployment across eleven rural health centers revealed something the lab data could never anticipate: variations in lighting and imaging equipment caused the system to reject more than 20% of images as unusable. Nurses had to repeat procedures multiple times. The throughput dropped to ten patients every two hours. The technology, rather than accelerating workflow, congested it.
What connects these three cases is not poor technical quality. It is the inability of the receiving organizations to absorb these tools without friction. And behind that inability is something deeper than an implementation failure. It is a structural mismatch that has been building for a long time.
The grammar medicine built and why it no longer holds
For centuries, medicine developed a sophisticated art of compressing biology into executable decisions.
Cholesterol: within range or above it. Triglycerides: normal or elevated. Hemoglobin: low or within normal values. TNM staging: T1, T2, T3, T4. Gleason score: 6, 7, 8, 9, 10. Disease stages: I, II, III, IV. Lab values: positive or negative, elevated or normal, inside or outside the threshold.
This is not a criticism. It is a description of something necessary and intelligent. Biology is continuous, multidimensional, and probabilistic. Medicine needs to act. To act, it needs to decide. To decide, it needs categories. So medicine built compression systems: tools for converting complex biological signals into discrete decisions that a physician can execute in the real time of a consultation, a night shift, a tumor board.
Electronic health records, for the most part, were designed with that same logic and with an additional purpose we rarely mention: to facilitate billing, not to optimize clinical reasoning. The result is an institutional infrastructure built to process low-dimensional decisions.
We are now asking that same infrastructure to metabolize something entirely different: spatial signatures of thousands of genes, multivariable tumor microenvironment scores, outputs from foundation models trained on millions of histological images.
And then we’re surprised when the system doesn’t respond.
Artificial intelligence and spatial biology don’t just generate more data. They generate data that no longer fits inside the compression systems medicine spent two centuries building. This is not a volume problem. It is a grammar problem. Medical organizations were designed to read a binary language. They are now receiving text written in a language with millions of dimensions.
The translation gap, in its most honest form, is this: the distance between the biological resolution at which we generate knowledge and the organizational capacity to interpret it, decide with it, and act in time.
The invisible cost no one is accounting for
There’s a conversation that happens rarely in papers and constantly in conference hallways: how much money dies in this gap.
Biomarker programs that fail to operationalize don’t disappear dramatically. They get archived. The team moves on to the next project. The data sits on a server. The finding, the one that could have better stratified patients, reduced Phase III failures, identified a responding subgroup, lives on as a PubMed paper that no one implemented.
The discovery didn’t die publicly. It died administratively.
The numbers are hard to calculate precisely, but the signals are clear: clinical trials that fail in Phase III because a biomarker stratification was never properly translated to the real world; companion diagnostics that obtain regulatory approval but never reach meaningful clinical adoption; digital pathology platforms deployed with multi-million dollar investments that pathologists abandon because they don’t fit into their workflow.
Each of these scenarios represents scientific capital, human capital, and financial capital invested in generating knowledge that never reaches its destination. And the most expensive part is not the money. It’s the time: the time that passes between discovery and clinical decision, during which patients continue receiving treatments that science had already learned to personalize better.
The true cost of the translation gap is not the failed pilots. It’s the generated knowledge that never became a better decision for a real patient.
The gap that lives inside your organization
I want to be specific about something that academic literature tends to treat abstractly.
In most mid-to-large biopharma organizations, the discovery team and the clinical development team operate under different logics, different incentives, and frequently, data systems that don’t communicate with each other. The discovery team optimizes for biological novelty. The clinical development team optimizes for regulatory executability. Between them exists a space (sometimes a chasm) where findings disappear.
It’s not just a communication problem between people, though that happens too. It’s that the data systems were not designed to talk to each other. The standards of the genomic research ecosystem and those of hospital information systems coexist without real interoperability in most institutions. The result: a finding identified with cutting-edge spatial transcriptomics cannot be directly converted into an executable medical order at the point of care.
This is the gap in its most concrete form. It is not philosophical, it is operational. And it lives in your data systems, in your information transfer processes between teams, in processing times that no one questions because they have always been that way.
The Python lesson and what translational medicine can learn from it
There’s a historical parallel I find useful, and it comes from a completely different domain: software.
In the early 2000s, Python was widely ignored and in some circles, actively dismissed. Major tech industries optimized for algorithmic performance: execution speed, computational efficiency, low-level hardware control. C++, Java, Fortran. Python, with its readable syntax and modest speed, was categorized as a beginner’s tool.
Twenty-five years later, Python is the foundation of nearly all artificial intelligence infrastructure. TensorFlow, PyTorch, scikit-learn, pandas, the entire ecosystem powering modern machine learning is built on Python. Why? Not because Python is the fastest language. Because Python optimizes the human, not the algorithm.
Python makes it easier for a scientist to think, explore, iterate, collaborate, and fail productively. And it turns out that is worth far more than the microseconds gained from a faster but less readable language.
Translational medicine faces exactly the same dilemma. For decades we have optimized for analytical precision: better models, higher resolution, stronger AUCs, more sophisticated platforms. And that matters. But translation, the act of converting a scientific finding into a clinical decision, may ultimately be a problem of human optimization.
The system that reaches the clinician at the right moment, with the right information, in a format that doesn’t interrupt their workflow, that leaves them in control and shows them the model’s uncertainty without pretending to have the final word, that system has a higher probability of changing a real decision than the most sophisticated algorithm in the world deployed on infrastructure that nobody uses.
What an organization that has crossed the gap actually looks like
I’ve observed that biomedical organizations tend to distribute themselves along a spectrum of what we might call information metabolism, their actual capacity to convert scientific signals into clinical decisions.
Some organizations accumulate signals, AI pilots proliferate in a fragmented way, each department manages its own data, and clinicians, overwhelmed by alerts with no response protocol, simply ignore the system. The result is chronic indigestion: growing IT costs, impressive committee presentations, and no real change in clinical practice.
Some organizations standardize signals, there is basic integration with clinical systems, data governance committees, models validated against recognized frameworks. The machinery works, but remains rigid. Findings arrive faster, but the system still doesn’t learn.
Some organizations operationalize signals, systems are embedded in closed decision loops with active human oversight. A concrete example is the Anemia Control Model, deployed across more than a hundred U.S. dialysis centers since 2013: it pulls hemoglobin trends directly from the EHR, calculates the optimal dose, and presents the suggestion inside the nephrologist’s standard prescribing workflow, approvable with a single click. A decade of evidence shows a sustained 25% reduction in unnecessary drug use and a 12% drop in hospitalizations. The system generates real clinical value because it was designed to operate inside the clinician’s reality, not alongside it.
And some organizations (still rare, but emerging) metabolize signals continuously. ARPA-H’s IGoR program points in that direction: infrastructure connecting computational modeling with experimental validation in cycles of under two weeks, where the organization doesn’t just use science, it produces it in real time. Synthetic metabolism: the state in which the translation gap stops being a structural problem and becomes a manageable process.
Most of the organizations we interact with (including large pharma companies) operate in the first two stages. Not for lack of scientific talent. For lack of the cognitive and sociotechnical infrastructure to make the transition.
What this means for those of us building these tools
If you develop biomarkers, lead translational medicine programs, or design digital pathology or spatial analysis platforms, this is the argument I want to leave with you:
The technical sophistication of your tool is necessary, but not sufficient. The real value of a biomarker is not in its AUC. It’s in whether it arrives on time at the right decision, inside the real system where it operates. And that system (with its processes, its data flows, its incentives, its response times, its action protocols) was not designed to receive it.
The work of closing the translation gap doesn’t start in the lab. It starts with the right question: who is going to use this result, at what point in their day, with what information available, and how much time do they have to act? If you don’t have a concrete answer to that question, the finding, however brilliant, is at high risk of ending up in the archive.
The cost of not asking that question is not abstract. It is measured in trials that fail because of incorrect stratification, in platforms abandoned because they don’t fit the workflow, in biomarkers that earn publication but never earn adoption. It is measured, ultimately, in the distance between what science already knows and what the patient already receives.
The organizations that will lead the next decade of biomedical innovation may not be the ones generating the most data. They will be the ones capable of metabolizing complexity faster than everyone else.
That is, at its core, what translational medicine is about. Not the movement of molecules from a lab to a clinic. The movement of decisions, from where they are generated to where they are needed.
References:
Kalyuzhny AE. Spatial Biology Evolution: Past, Present and Future of Mapping Life in Context. Cells. 2026 Apr 22;15(9). doi:10.3390/cells15090743
Leaders OT. The “Pilot Purgatory”: Why 80% of Pharma AI Projects Fail (And How to Fix It) [Internet]. 2026 Feb 16 [cited 2026 May 22]. Available from: https://hitconsultant.net/2026/02/16/cloudera-life-sciences-ai-scalability-pilot-failure-roi/
Li J. Bridging the Precision Gap: Accelerating Clinical Adoption of Companion Diagnostics in Oncology | PharmExec [Internet]. 2026 [cited 2026 May 22]. Available from: https://www.pharmexec.com/view/bridging-precision-gap-accelerating-clinical-adoption-companion-diagnostics-oncology
Hospitals Grapple With AI Health Accuracy Crisis. AI CERTs News [Internet]. [cited 2026 May 22]. Available from: https://www.aicerts.ai/news/hospitals-grapple-with-ai-health-accuracy-crisis/
When Algorithms Fail: Preparing for AI Incidents in Clinical Settings | Censinet, Inc. [Internet]. [cited 2026 May 22]. Available from: https://censinet.com/perspectives/when-algorithms-fail-preparing-ai-incidents-clinical-settings
Alsentzer E, Charpignon ML, Chen B, D’Souza N, Fries J, Jiang Y, et al. Reflections from Research Roundtables at the Conference on Health, Inference, and Learning (CHIL) 2025 [Internet]. arXiv; 2025 [cited 2026 May 22]. Available from: http://arxiv.org/abs/2510.15217 doi:10.48550/arXiv.2510.15217
RFP.wiki [Internet]. [cited 2026 May 22]. Atomwise - Cost Drivers: Pricing & Contracts (2026). Available from: https://www.rfp.wiki/artificial-intelligence/ai-drug-discovery-platforms/atomwise
Pharm.D MN. Minimize your clicks, maximize your time: 5 common EHR mistakes that slow medical practices | Medical Economics [Internet]. 2026 [cited 2026 May 22]. Available from: https://www.medicaleconomics.com/view/minimize-your-clicks-maximize-your-time-5-common-ehr-mistakes-that-slow-medical-practices
MPH BT MD. [AI Deployment in Healthcare: Why Most Prototypes Fail]{.chapter-title} [Internet]. doi:10.5281/zenodo.18263442
Cheungpasitporn W, Athavale A, Ghazi L, Kashani KB, Colicchio T, Koyner JL, et al. Transforming nephrology through artificial intelligence: a state-of-the-art roadmap for clinical integration. Clin Kidney J. 2026 Feb 1;19(2):sfag004. doi:10.1093/ckj/sfag004
Granted AI [Internet]. 2026 [cited 2026 May 22]. ARPA-H Bets on AI-Generated Hypotheses: Inside the IGoR Program’s Plan to Build Mechanistic Disease Models. Available from: https://grantedai.com/blog/arpa-h-igor-intelligent-generator-research-ai-biomedical-disease-models-strategy-2026